68YEAR OLD FEMALE WITH SHORTNESS OF BREATH
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis .
COMPLAINTS AND DURATION:
-Patient c/o cough since 6 months
-Shortness of breath since 4-5 months
HISTORY OF PRESENTING ILLNESS:
-Patient was apparently normal until 6months back,then she developed
-Productive cough, insidious in onset, gradually progressive with white colored mucoid sputum, relieved on taking medication and aggravated mostly at night time around 3-4AM-Shortness of breath: since 4-5 months, insidious in onset and gradually progressed to grade-IV now.
-Orthopnoea present, feels better on lying to lateral side, patient also gives h/o PND
No H/O fever, burning micturition, pain abdomen, chest pain, palpitations, decreased urine output, pedal edema.
PAST HISTORY:
-H/o decreased appetite since 4 months.
-No h/o fever/ burning micturition/ pain abdomen / chest pain/ palpitations.
No Decreased urine output/ pedal edema.
-Not a k/c/o DM/HTN/TB/ Epilepsy / CVA / CAD/ thyroid diseases
- H/o fall 2 years back - Right ankle # - POP applied.
PERSONAL HISTORY:
-Normal appetite, mixed diet with regular bowel and
bladder habits
-Addiction of smoking :
2-3beedis/day started 8years back ,stopped 2 years
back.
GENERAL EXAMINATION:
PT IS C/C/C
PALLOR: PRESENT
NO ICTERUS, CYANOSIS, CLUBBING, PEDAL EDEMA, LYMPHADENOPATHY.
VITALS ON ADMISSION:
PR-96BPM
BP- 120/70MM HG
RR- 20CPM
SPO2- 99% AT RA
SYSTEMIC EXAMINATION:
CVS:
S1 S2 PRESENT
NO THRILLS AND NO MURMURS
RESPIRATORY SYSTEM:
INSPECTION:
CHEST IS BILATERALLY SYMMETRICAL
TRACHEA MIDLINE IN POSITION
APICAL IMPULSE NOT APPRECIATED
CHEST IS MOVING NORMALLY WITH RESPIRATON NO DIALTED VEINS, SCARS, SINUSES.
PALPATION:
TRACHEA MIDLINE IN POSITION
APICAL IMPULSE FELT ON 5TH INTERCOASTAL SPACE
CHEST IS MOVING EQUALLY WITH RESPIRATION ON BOTH SIDES.
PERCUSSION:
ON PERCUSSION RESONANT NOTE HEARD.
AUSCULTATION:
NORMAL VESICULAR BREATH SOUNDS HEARD NO ADVENTITIOUS SOUNDS HEARD.
ABDOMEN:
SHAPE OF ABDOMEN: SCAPHOID NO TENDERNESS
NO PALPABLE MASSES
NO FREE FLUID AND NO BRUITS LIVER IS NOT PALPABLE
SPLEEN NOT PALPABLE
BOWEL SOUNDS:PRESENT
CNS:
HIGHER MENTAL FUNCTIONS- INTACT
MEMORY- ABLE TO RECOGNISE HIS FAMILY MEMBERS AND RECALL RECENT EVENTS SPEECH: NORMAL
CRANIAL NERVE EXAMINATION- NORMAL REFLEXES-
RIGHT LEFT
BICEPS 2+ 2+
TRICEPS 2+ 2+
SUPINATOR 1+ 1+
KNEE 2+ 2+
ANKLE. 2+ 2+
SUPERFICIAL AND DEEP REFLEXES ARE PRESENT AND NORMAL
MUSCLE POWER-
RIGHT LEFT
UPPER LIMB
ELBOW 5/5 5/5
WRIST 5/5 5/5
HAND GRIP 5/5 5/5
LOWER LIMB
HIP 5/5 5/5
KNEE. 5/5 5/5
ANKLE 5/5 5/5
TONE- NORMAL IN UPPER AND LOWER LIMBS
NO INVOLUNTARY MOVEMENTS
SENSORY SYSTEM- ALL SENSATIONS ARE NORMAL
INVESTIGATIONS:
Hb- 10.7gm/do
TLC-7900cells/cu.mm
PLT-2.04lakhs/cu.mm
Creatinine- 0.8mg/dl
Urea- 22mg/dl
RBS- 101mg/dl
LFT
TB- 0.76mg/dl
DB- 0.20mg/dl
AST-19IU/L
ALT-16IU/L
ALP- 142 IU/L
TP- 6.7gm/dl
ALB- 3.3gm/dl
Na- 141
K- 3.6
Cl- 99
Ca- 0.9
Serology- negative
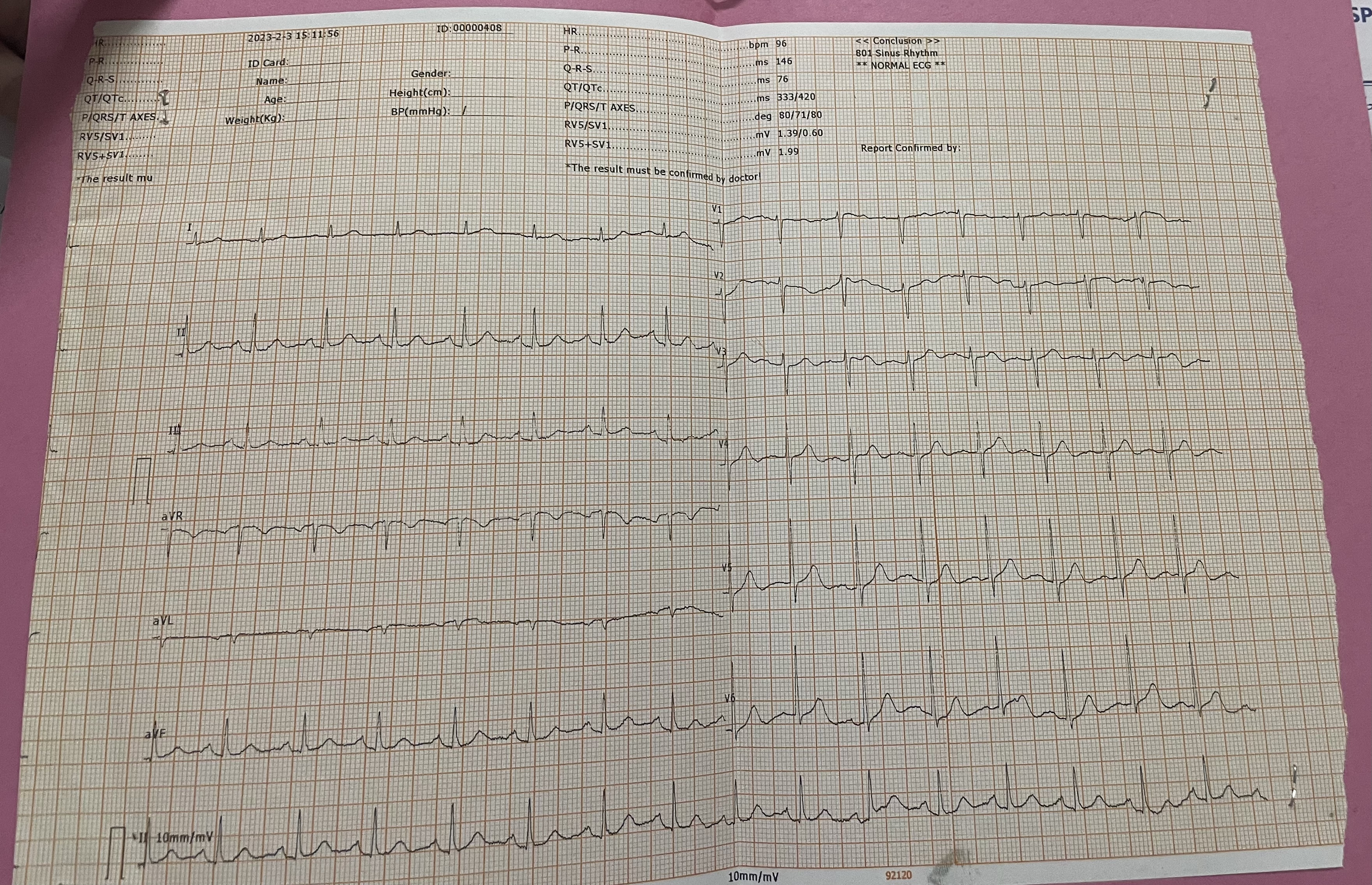
ECG
CHEST X-RAY

SPUTUM CULTURE AND SENSITIVITY: Normal oropharyngeal flora grown.
2D ECHO -
IMPRESSION: TRIVIAL TR+/AR+, NO MR
NO RWMA, NO AS/MS
GOOD LV SYSTOLIC FUNCTION DIASTOLIC DYSFUNCTION
NO PAH/PE
SPUTUM CBNAAT - NEGATIVE.
TREATMENT:
1. SYRUP ASCORYL 2 TSP TID X 12DAYS
2. TAB LEVOCETRIZINE 5MG PO BD X 12 DAYS
3. TAB PAN 40MG PO OD X 12 DAYS
4. NEBULISATION WITH DUOLIN 4TH HOURLY , BUDECORT 12TH HOURLY. X 12 DAYS
5. SYP. CREMAFFIN 10ML PO HS X 9DAYS
ADVICE AT DISCHARGE:
1. SYRUP ASCORYL 2 TSP TID
2. TAB LEVOCETRIZINE 5MG PO BD
3. TAB PAN 40MG PO OD
4. INHALERS WITH DUOLIN 4TH HOURLY , BUDECORT 12TH HOURLY.
5. SYP. CREMAFFIN 10ML PO HS



Comments
Post a Comment