14 YEAR OLD FEMALE WITH FEVER
SUDHAMSHI REDDY
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis


SYSTEMIC EXAMINATION:
RS: BAE ,NVBS, no added sounds
CVS : S1 ,S2 heard no murmurs
P/A : soft , non tender

CNS:
HIGHER MENTAL FUNCTIONS- INTACT
MEMORY- able to recognise her family members and recall recent events
SPEECH: normal
CRANIAL NERVE EXAMINATION- normal
REFLEXES-
RIGHT LEFT
BICEPS 3+ 3+
TRICEPS 2+ 2+
SUPINATOR 1+ 1+
KNEE 2+ 2+
ANKLE. 2+ 2+
SUPERFICIAL AND DEEP REFLEXES ARE PRESENT AND NORMAL
MUSCLE POWER-
RIGHT LEFT
UPPER LIMB
ELBOW 5/5 5/5
WRIST 5/5 5/5
HAND GRIP 5/5 5/5
LOWER LIMB
HIP 5/5 5/5
KNEE. 5/5 5/5
ANKLE 5/5 5/5
TONE- NORMAL IN UPPER AND LOWER LIMBS
NO INVOLUNTARY MOVEMENTS
SENSORY SYSTEM- ALL SENSATIONS ARE NORMAL
Referred to dermatology I/V/O itching all over the body, was diagnosed as scabies and adviced
1. PERMETHRIN 5% LOTION LA ON DAY1, DAY 8
2. Tab. TECZINE 5mg SOS.
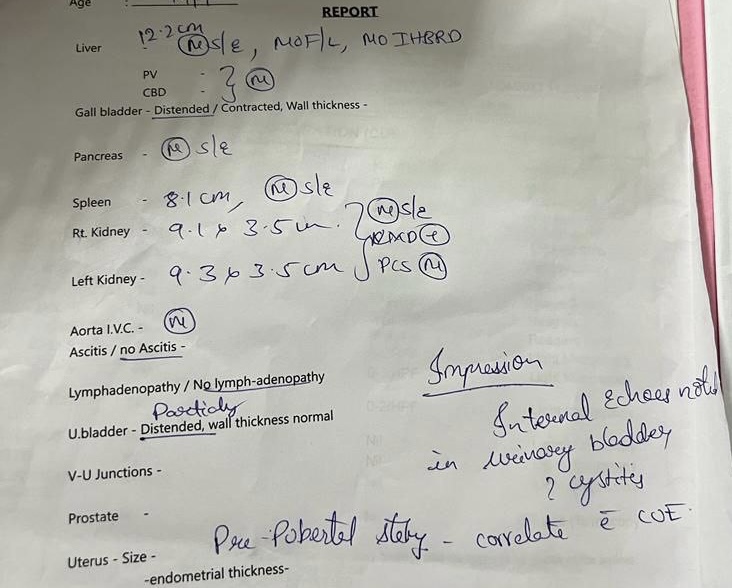


PROVISIONAL DIAGNOSIS:
VIRAL PYREXIA WITH CHRONIC CYSTITIS
TREATMENT:
1.TAB PCM 500mg PO/SOS
2. SYP ASCORIL LS PO/ TID
3. SYP CITRALKA 10ml PO/TID in 1 glass of water
4. PERMETHRIN 5% LOTION LA
5. TAB TECZINE 5mg PO/SOS


Comments
Post a Comment