60 YEAR OLD MALE WITH PAIN ABDOMEN
SUDHAMSHI REDDY M
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis
60 year old male came with complaints of
Pain abdomen since 3 days
Vomitings since 2 days
HOPI:
Patient was apparently asymptomatic 1 year ago, from then he had pain abdomen once a month for which he consulted local doctor and took treatment.
Patient now presented with complaints of pain abdomen since 3 days- Umbilicus, left hypochondrium and left lumbar region.
Non radiating,pain is severe and relieved on bending forward.
Vomitings since 2 days- 3 episodes/ day, food particles as content, non bilious, non projectile, not blood stained.
No H/O fever, loose stools.
PAST HISTORY:
Not a K/C/O HTN, DM,TB, ASTHMA,EPILEPSY,THYROID DISORDERS.
PERSONAL HISTORY:
Appetite normal
Diet mixed
Sleep normal
Bowel and bladder regular
Alcoholic consumes 90ml daily
Smoker- stopped 3 years ago.
GENERAL EXAMINATION:
Patient is conscious, coherent ,cooperative
Afebrile on touch
PR : 88bpm
RR : 20cpn
BP : 140/90mm of hg
Spo2: on 97% on RA
Grbs : 183mg/dl
SYSTEMIC EXAMINATION:
RS: BAE NVBS no added sounds
CVS : S1 S2 heard no murmurs
P/A : soft , non tender

CNS : higher mental functions intact
Tone normal in all 4 limbs
Power 5/5 in all limbs
All reflexes present
INVESTIGATIONS:
Hb- 16
PCV- 50.1
TLC- 15,700
PLT- 1.56
Blood urea-44
Serum creatinine- 1.4
Na- 137
K- 4.3
CL-102
LFT
Tb- 1.84
Db- 0.75
SGOT-65
SGPT-29
ALP- 223
TP- 7.3
ALB- 3.63
A/G- 0.99
CUE- albumin+
Serum amylase- 650
Serum lipase- 238
USG ABDOMEN-
Impression:
-Pancreas head appears bulky measuring 20mm with heterogenous echo texture
-Rest of pancreas is obscured by bowel gas likely Acute pancreatitis
- Visualised bowel loops appears normal and not dilated.
CXR-

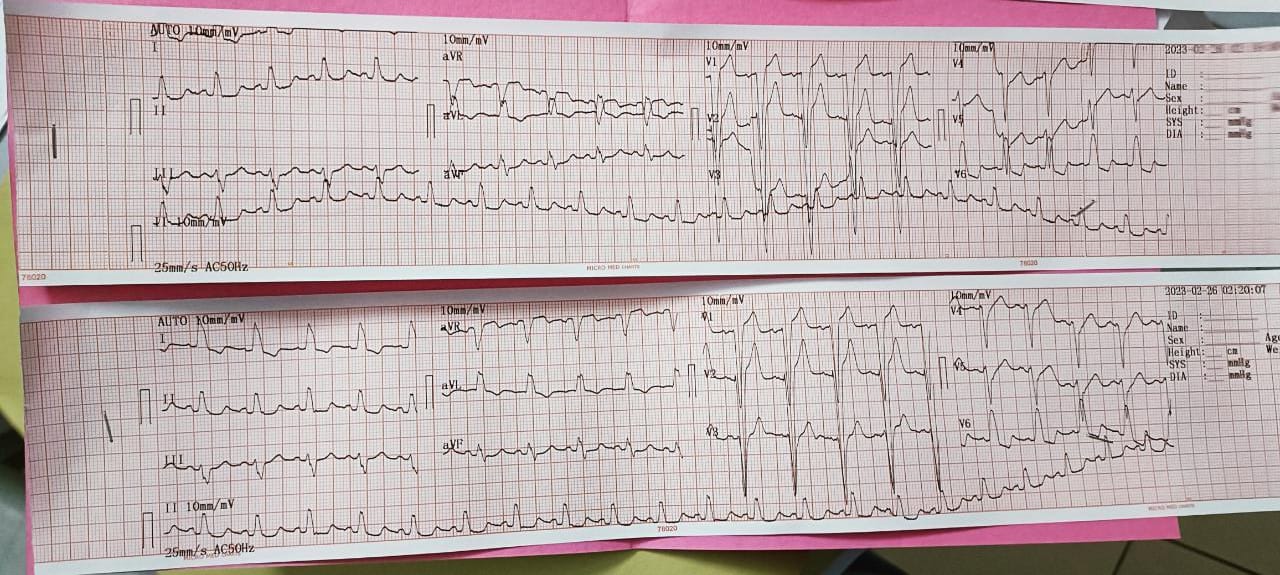
ECG-
PROVISIONAL DIAGNOSIS:
ACUTE PANCREATITIS
TREATMENT:
1. NBM TILL FURTHER ORDERS
2. IVF 1 UNIT RL
1 UNIT NS
1 UNIT DNS @ 100ml/hr
3. INJ TRAMADOL 1AMP IN 100ml NS IV TID
4.INJ THIAMINE 200mg in 100ml NS TID.



Comments
Post a Comment